* The content of this article is intended for a medical and veterinary audience due to graphic images of surgical procedures.
Patient
1 year old Ridgeback
Complaint
The canine patient required a shoulder arthrodesis due to lameness from trauma induced osteoarthritis as a puppy.
Brief
The patients joint needed to be fused at 110 degrees of shoulder flexion.
Anatomical Models
The specification prescribed by the consultant surgeon clarified that two anatomical models were required. The first model to be printed directly from the original CT scan data so that they could rehearse the surgery on it.
For the second model they wanted the print of the limb at 110 degrees and within the osteotamies already performed, joint surfaces removed and bones reduced to pre-contour the plates pre-op to save surgical time.

Surgical Guides
To work alongside the anatomical models, they also requested two guides to aid the surgery. A cutting guide was designed to attach onto and span the scapula and humerus to allow osteotomy cuts to occur at the bottom of each of these bones to remove the joint surface so that they aligned perfectly with each other.
A repositioning guide was designed to aid the osteotomy cuts into their new 110 degree of shoulder flexion. The guide held the bones into its reduced position whilst they started to place the pre-contoured plates.

The Surgery
For both surgical guides 2.0mm diameter K wires were used to position onto the scapula and humerus. The K wires were placed into both bones during the use of the cutting guide. Once the cuts were made the cutting guide was removed leaving the four K wires in situ (two in the scapula accutane and two in the humerus).
The repositioning guide was placed onto the two upper scapula K wires. The two lower humerus K wires and humerus was rotated into its new position.The lower K wires fixated into the lower half of the repositioning guide to hold it steady until the plates were screwed into their correct pre-contoured position.
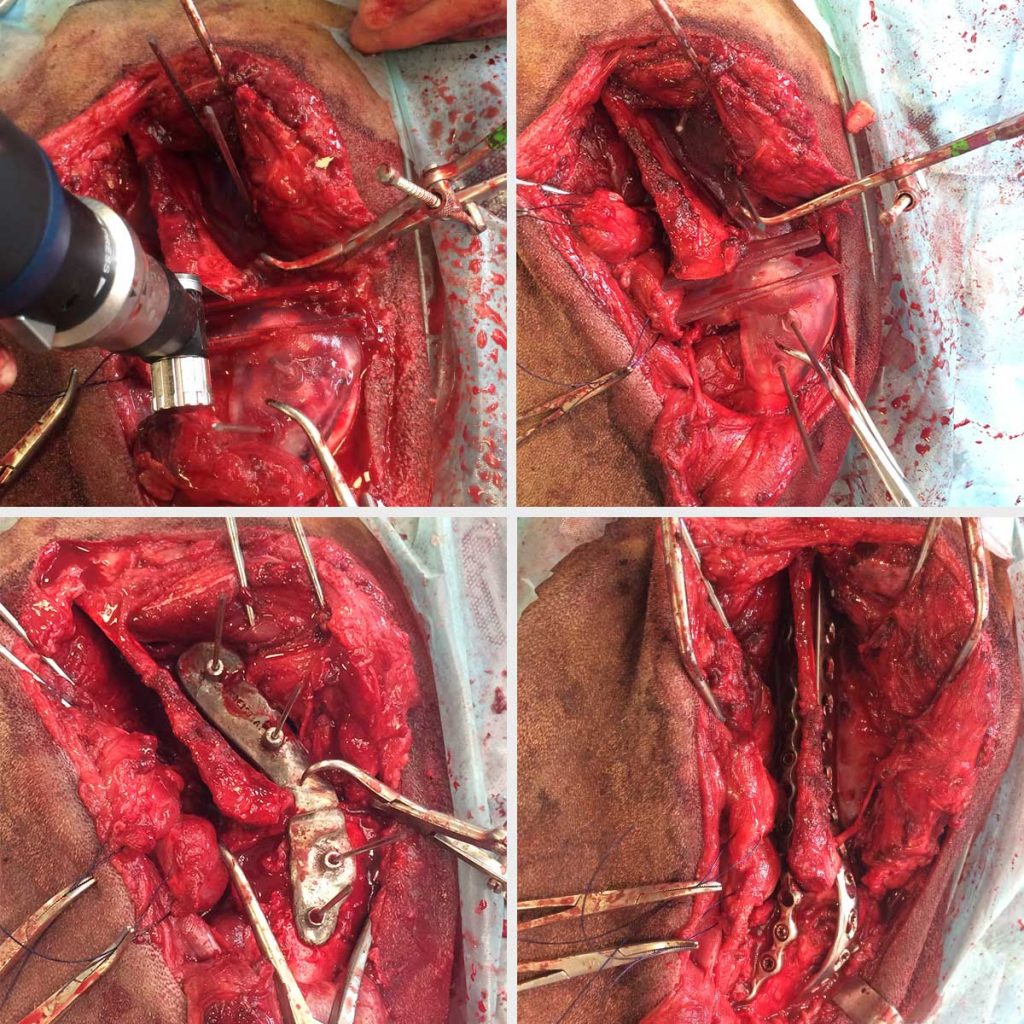
“The cutting guide worked really nicely, I’m really happy with the orientation of the osteotomies and the reduction of the bone prior to plating. On the craniocaudal radiograph the limb is also bullet straight which is what I wanted to achieve.”
Consultant Surgeon